
The Ebola outbreak 2026 in the Democratic Republic of the Congo has rapidly escalated into a global health emergency, with the World Health Organization declaring it a Public Health Emergency of International Concern. Suspected cases have now climbed to 600, with 139 suspected deaths, as the WHO Emergency Committee confirmed the virus remains a serious public health threat at the national and regional levels. The Ebola outbreak in Africa has already crossed into Uganda and led to the first intercontinental medical evacuation of an infected American doctor.
Background: Where Does Ebola Come From?
Understanding where Ebola comes from is essential to tracking how outbreaks begin. Ebola disease was first identified in 1976 after an outbreak in what is now the Democratic Republic of the Congo. Since then, these viruses have periodically emerged from an unknown animal host and infected people in several African countries.
Ebola viruses are zoonotic, meaning they are carried naturally by animals. Occasionally, the viruses “spillover” into the human population, where they can spread easily from person to person. Scientists believe fruit bats are the most likely natural reservoir, though the exact mechanism of the first human infection in any given outbreak remains under investigation.
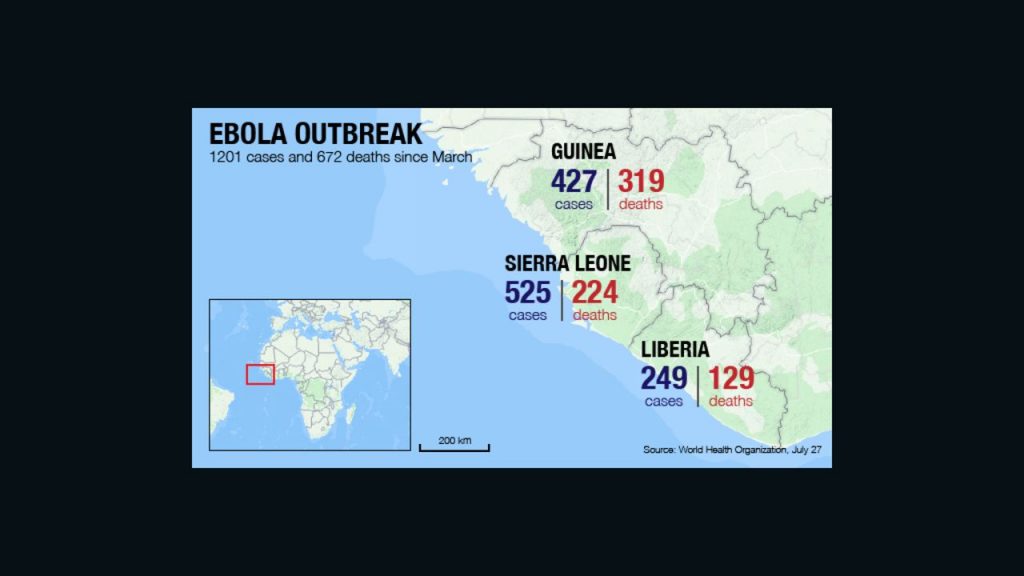
The Ebola outbreak 2014 serves as a grim reference point. That West Africa epidemic, caused by the Zaire strain of Ebola, lasted two years and killed over 11,000 people. The 2014–2016 West Africa outbreak alone accounts for about 80 percent of the cumulative Ebola case total since 1976, with Sierra Leone, Liberia, and Guinea carrying the heaviest burden.
The Ebola Outbreak 2026: How It Started
The Democratic Republic of Congo declared its 17th Ebola outbreak on May 15, 2026, after cases were confirmed in Ituri Province a region already heavily affected by conflict, displacement, hunger, and limited access to healthcare, all of which make it harder to stop the spread of disease.
In early May, a hospital in Bunia Health Zone in northeastern DRC identified a cluster of severe illnesses affecting healthcare workers. Initial samples tested in DRC were negative for Ebola virus, but by May 15, eight out of 13 samples tested positive, and five were inconclusive. Using genetic fingerprinting, the illnesses were identified as Bundibugyo virus one of the four types of orthoebolaviruses that cause Ebola disease in people.
WHO experts believe the outbreak began a few months ago, with the first suspected death reported on April 20. After that first death, a suspected super-spreader event is believed to have taken place at either a funeral or a healthcare facility, though investigations are ongoing.
Ebola Outbreak 2026 Map: Where Is It Spreading?
The Ebola outbreak 2026 map tells a story of rapid and widening geographic spread. The confirmed cases in DRC have been reported from Ituri and North Kivu provinces, including cases in the capitals Bunia and Goma. A case has also been confirmed in South Kivu Province in a person who had traveled from Tsopo Province.
As of May 21, 2026, the Ebola Bundibugyo outbreak in DRC has been reported in 11 health zones in Ituri Province and in Nord-Kivu Province. This rapid expansion across multiple health zones is a key reason the WHO upgraded the situation to its highest alert level.
Two laboratory-confirmed cases with no apparent link to each other were reported in Kampala, Uganda, within 24 hours of each other on May 15 and 16, 2026, among two individuals who had travelled from the DRC. The cross-border spread pushed the Ebola outbreak in Africa beyond DRC’s borders for the first time in this episode.
How Does Ebola Spread?
One of the most critical public questions surrounding the Ebola outbreak 2026 is: how does Ebola spread? The answer matters for both containing the outbreak and managing public fear.
The Bundibugyo virus spreads easily through blood and other bodily fluids, as well as contaminated surfaces. Handling dead bodies is also a known risk for the spread of the virus. Traditional funeral practices that involve direct contact with the deceased have been linked to multiple outbreaks historically.
A person infected with an orthoebolavirus is not considered contagious until after symptoms appear. Early “dry” symptoms include fever, aches, pains, and fatigue, while later “wet” symptoms include diarrhea, vomiting, and unexplained bleeding.You cannot get Ebola from simply being near someone or passing them in public spaces, because it does not spread through the air. This is a critical distinction that separates Ebola from respiratory viruses like influenza or COVID-19, and is why public risk in distant countries remains low.
Ebola Symptoms: What to Watch For
Ebola symptoms in the 2026 outbreak follow the same pattern seen in previous outbreaks, though their variability makes early diagnosis particularly difficult.
Patients have experienced classic Ebola disease symptoms including fever, headache, vomiting, severe weakness, abdominal pain, nosebleeds, and vomiting blood. These symptoms typically appear between two and 21 days after exposure.
Like other Ebola viruses, Bundibugyo causes flu-like symptoms fever, muscle aches, and fatigue that often progress to severe diarrhea, vomiting, and bleeding. Symptoms vary enough from person to person that infections can often be mistaken for malaria or typhoid if diagnostic testing is not done.This diagnostic confusion is one of the key reasons the Ebola outbreak 2026 was not identified sooner. In a region where malaria is endemic and health infrastructure is stretched, Ebola can circulate for weeks before it is formally detected.
Quotes: What Experts Are Saying
WHO Director-General Tedros Adhanom Ghebreyesus stated: “The WHO assesses the risk of the epidemic as high at the national and regional levels and low at the global level,” while confirming the virus remains a Public Health Emergency of International Concern but not yet a pandemic emergency.
Dr. Geeta Sood, a hospital epidemiologist at Johns Hopkins Bayview Medical Center, noted the Bundibugyo virus carries a mortality rate of around 25 to 40 percent lower than other types of Ebola, which average around 50 to 60 percent. The mortality rate for the Zaire type, the most common species, is 60 to 90 percent.
Dr. Satish Pillai, head of the CDC’s Ebola response, confirmed during a media briefing that there are no cases in the United States and the threat to the American public “remains low.”
Will Ebola Become a Pandemic?
The question of whether Ebola will become a pandemic is front of mind for many following the Ebola outbreak 2026. Public health experts are cautiously reassuring but alert.
The WHO determined that while the Ebola disease outbreak in DRC and Uganda constitutes a Public Health Emergency of International Concern, it does not meet the criteria of a pandemic emergency as defined in the International Health Regulations.
The outbreak is occurring in areas affected by insecurity, population displacement, mining-related population movement, and frequent cross-border travel, all of which may increase the risk of further transmission. These factors make containing the outbreak difficult but do not automatically translate into global pandemic risk.
On May 18, 2026, the CDC and DHS implemented enhanced travel screening, entry restrictions, and public health measures to prevent Ebola virus disease from entering the United States amid the ongoing outbreaks in East and Central Africa.
Impact: Regional and Global Consequences
The Ebola outbreak in Africa is already generating consequences well beyond DRC’s borders. An American missionary doctor Peter Stafford, infected while treating patients at Nyankunde Hospital near Bunia was airlifted to Berlin’s Charité hospital for treatment in its high-security isolation unit. His wife and four young children were also evacuated to the same hospital.
The Ebola outbreak 2026 is also straining an already overloaded healthcare system. The virus remains contagious for up to three days after a victim dies, which is why burial practices can contribute to new cases spreading. Patients who receive early treatment have a higher chance of survival and are less likely to infect others.
For the Ebola outbreak 2026 map to stop expanding, international response teams must overcome severe logistical obstacles. The outbreak zone in Ituri is a gold-mining region with high population mobility, armed conflict, and limited road access conditions that historically make Ebola containment extremely difficult.
Conclusion: What Comes Next
The Ebola outbreak 2026 is not yet contained, and the trajectory over the coming two to three weeks will be decisive. This outbreak involves the Bundibugyo strain, a type of Ebola for which there is currently no approved vaccine, making early supportive treatment, contact tracing, and isolation the primary tools available to health workers.
The WHO and Africa CDC are both on high alert, and international partners including the CDC, Médecins Sans Frontières, and the International Rescue Committee have deployed teams to the ground. Whether the Ebola outbreak in Africa can be contained within DRC and Uganda, or whether it spreads further, depends heavily on the speed and scale of this coordinated response.
Public health authorities stress that understanding how Ebola spreads, recognizing Ebola symptoms early, and following official guidance are the three most important tools the public has in the face of this growing crisis.
FAQs
What is the famous book about Ebola?
The most widely read book about Ebola is The Hot Zone by Richard Preston, published in 1994. It chronicles the emergence of the Ebola Reston virus in a primate research facility near Washington D.C. in 1989 and provides a gripping account of how the virus behaves in the human body. Another significant work is Spillover by David Quammen, which explores the science of zoonotic diseases including Ebola and explains how viruses jump from animals to humans the central question behind every Ebola outbreak in Africa.
What are the four types of Ebola? There are four species of orthoebolaviruses known to cause illness in people. The first is the Zaire Ebola virus the most common and most lethal, responsible for the devastating Ebola outbreak 2014 in West Africa and the basis for the only currently approved Ebola vaccine. The second is the Sudan Ebola virus, which has caused multiple outbreaks in Uganda and Sudan. The third is the Bundibugyo virus the strain driving the Ebola outbreak 2026 in DRC and Uganda which was first discovered in Uganda in 2007 and has no approved vaccine or treatment. The fourth is the Taï Forest virus, which has caused only a single known human infection. A fifth species, Reston virus, affects primates but has not been confirmed to cause disease in humans.
Who was the woman who stopped Ebola?
Dr. Joanne Liu, former International President of Médecins Sans Frontières (Doctors Without Borders), is widely credited as one of the most important figures in bringing the catastrophic Ebola outbreak 2014 under control. In September 2014, she delivered a landmark address at the United Nations in Geneva, warning world leaders that the outbreak was “out of control” and demanding the immediate deployment of civilian and military medical assets to West Africa. Her forceful advocacy is widely seen as the turning point that galvanized international action and accelerated the response that eventually ended the epidemic. Dr. Liu’s experience directly shaped how the world approaches Ebola outbreak in Africa responses today.